ADHD
These are links to help people with disabilities cut down on the emotional labour of self-advocacy. This page can help you understand what ADHD is, how it presents differently across people and contexts, and how to be a genuine ally to someone who has it.
Before You Continue
A few concepts do a lot of work on this page. If any of these are new to you or you haven’t engaged with them recently, they are worth the refresher.
- Masking — Why performing neurotypicality is not a neutral ask, and what it costs over time
- Spoon Theory — Why energy depletion in ADHD is not a matter of effort or willpower
- Ableism — Why the standard responses to ADHD traits are often a structural problem, not a character one
- Reasonable Accommodations — What support actually looks like in practice
Language
The ADHD community generally prefers Person First Language (PFL), which places personhood before diagnosis.
| Instead of | Prefer |
|---|---|
| ADHDer | Person with ADHD |
| ADHD kid | Child with ADHD |
The logic is the same as preferred usage in oncology: a person with cancer is not defined by their diagnosis. Person first language reflects that a diagnosis is one descriptor among many, not the whole person.
What ADHD Actually Is
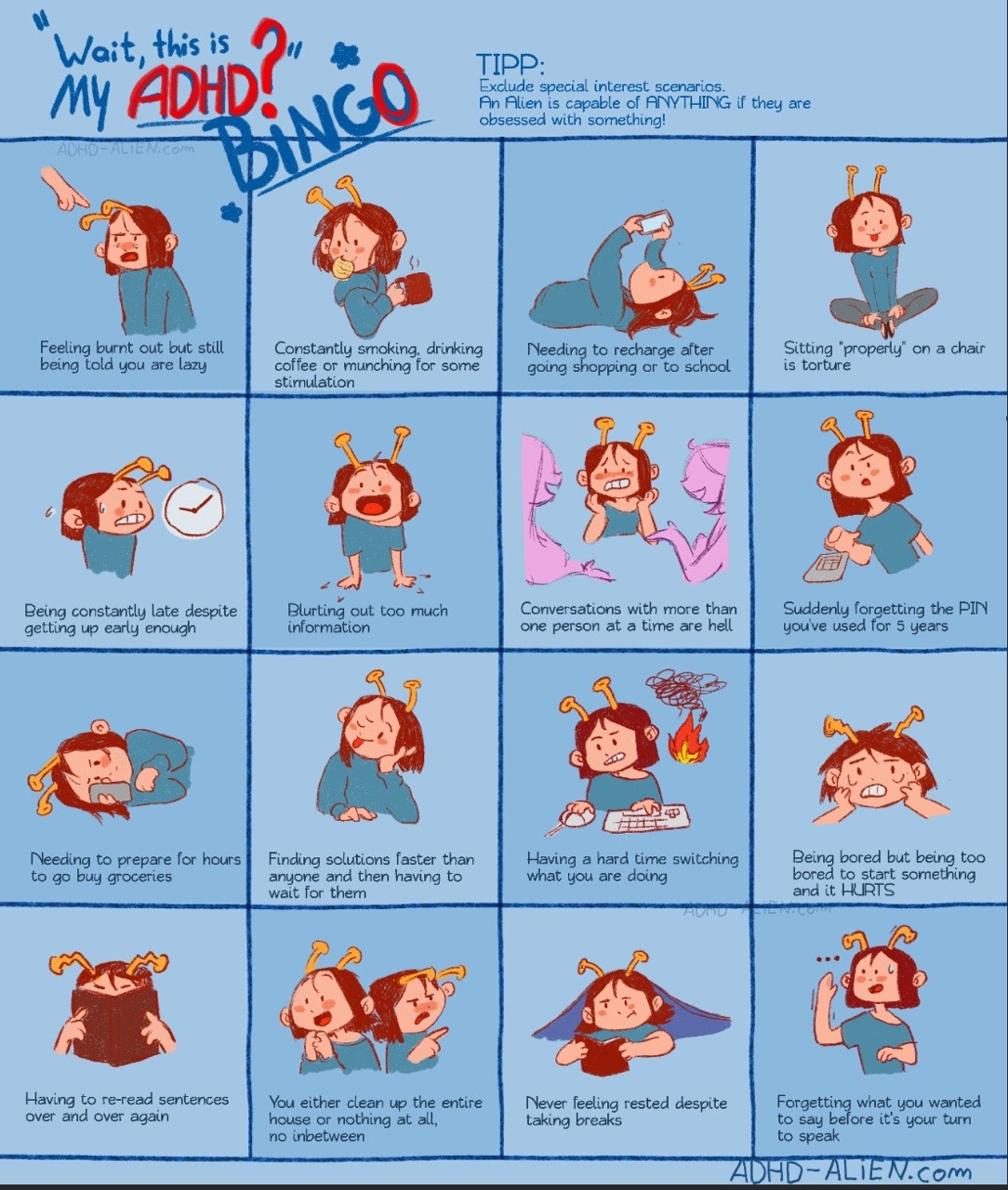
ADHD is a neurodevelopmental condition characterized by differences in attention regulation, impulse control, and executive functioning. The name is somewhat misleading: people with ADHD do not have a deficit of attention so much as a different relationship to it. Hyperfocus the ability to sustain intense, prolonged concentration on something intrinsically motivating is as characteristic of ADHD as distractibility. The difference is that the regulation is less voluntary.
The condition is also significantly more complex than its common representations suggest. ADHD presents across three subtypes: (1) inattentive, (2) hyperactive, and (3) combined, and its expression varies considerably by age, gender, co-occurring conditions, and environment. What looks like ADHD in a seven-year-old boy in a classroom is often not what ADHD looks like in a thirty-five-year-old woman in a professional setting, and the diagnostic criteria were built largely around the former.
The Executive Function Picture
Executive functioning is the set of cognitive processes that manage goal-directed behaviour: planning, initiating, prioritizing, shifting attention, regulating emotion, and holding information in working memory while using it. ADHD affects all of these to varying degrees, which is why its impact extends well beyond concentration.

A person with ADHD may be able to write a sophisticated analysis of a complex topic and be entirely unable to send a routine email on the same day. These are not contradictions. They reflect the role of interest, urgency, novelty, and challenge in regulating the ADHD nervous system, what researcher William Dodson has described as an interest-based nervous system rather than a priority-based one. The task is not too hard. It is too boring, too unstructured, or too disconnected from anything that activates engagement.
This distinction matters because the standard response to missed tasks, forgotten deadlines, and inconsistent output is to assume insufficient effort. The intervention that follows is pressure, which produces shame, which makes the executive dysfunction worse. The cycle is as predictable as it is counterproductive.
ADHD in Women and Girls
Because early research on ADHD was conducted almost exclusively with boys, the diagnostic criteria reflect a presentation that is more common in male-typical ADHD: visible hyperactivity, impulsivity, and external disruptiveness. Girls and women with ADHD are more likely to present with inattentive symptoms, internal restlessness, chronic disorganization, emotional dysregulation, and extensive masking, which are both less visible and less legible to the diagnostic framework.

The consequences of this gap are significant. Women with ADHD are more likely to receive incorrect diagnoses, anxiety, depression, personality disorders, before anyone identifies the underlying condition. They grow up being described as scattered, oversensitive, or underachieving without ever being given the framework that would make sense of their experience. By the time many receive a correct diagnosis, they have spent decades building elaborate compensatory strategies that work just well enough to hide how much effort everything costs.
Dismissal compounds the difficulty. A woman who has been told she is disorganized, rather than that she has a condition affecting executive function, does not receive tools. She receives judgment. The difference in outcome is not subtle.
ADHD and Social Life
The social dimension of ADHD is one of its least discussed and most consequential features. Differences in time perception, working memory, emotional regulation, and impulse control all have direct effects on how relationships form and are maintained, and the social feedback that accumulates over years of missed cues, forgotten follow-ups, and unfiltered honesty shapes how a person with ADHD understands their own social worth.
One of the most significant patterns is what friendship researcher and coach Caroline Maguire, who works specifically with neurodivergent adults, identifies as the “take what you can get” mindset. People with ADHD who have experienced repeated social rejection or marginalization often internalize the belief that they have no standing to choose their friends, that if someone will accept them, they should be grateful and stop there. This is not a personality trait. It is the logical conclusion of growing up in environments where the pool felt small and the social cost of being yourself was high.

The problem is that friendship built on this foundation tends to confirm the belief that drove it. When you invest in relationships that aren’t a genuine fit, friendship feels like a burden. The effort is high and the return is low. The conclusion that follows, that connection doesn’t work for people like you, is wrong, but it is understandable given the evidence.
The shift Maguire describes is not about becoming more demanding. It is about starting with a different question: not who will accept me but who do I actually want to spend time with, doing things I actually enjoy? This reorientation, from scarcity to curation, is one of the more significant moves available to neurodivergent adults who have spent years in friendships that were more obligation than connection.
ADHD and the Cultural Context
ADHD does not exist in a vacuum. Its impact is shaped significantly by the demands of the environment, and Western, industrialized, highly individualistic societies are unusually demanding environments for people whose nervous systems work the way ADHD nervous systems do.
The premium placed on independent productivity, consistent output, linear task management, punctuality, and sustained concentration maps almost precisely onto the areas most affected by ADHD. These are not universal human values. They are the values of a particular economic arrangement, and they happen to function as a filter that systematically disadvantages people with ADHD, particularly those without access to supportive structures.
Many non-Western contexts build the kind of communal scaffolding: extended family networks, shared domestic labour, flexible social rhythms, that naturally compensates for executive function differences. The person who struggles to maintain a household alone may thrive within a structure where those tasks are distributed. The person who finds rigid scheduling suffocating may perform well within a culture where time is understood differently. These are not anomalies. They are evidence that what reads as impairment in one context is often a mismatch between a nervous system and an environment.
What Support Actually Looks Like
ADHD is not addressed by trying harder. It is addressed by building systems that work with how the brain actually functions rather than demanding it function differently.
Some of what this looks like in practice: automating recurring tasks so they don’t require initiation, using external structure to compensate for internal time blindness, communicating directly about how you work so that others know what to expect rather than inferring it, and building in recovery time after high-demand periods rather than treating depletion as a personal failure.
The distinction between adapting and masking is worth naming here. Adapting is chosen, skill-based, and functional. It means finding workarounds that reduce friction without requiring you to perform a version of yourself that isn’t real. Masking is compelled, chronic, and costly. It means suppressing the signals your nervous system produces in order to appear more neurotypical, and it is directly associated with burnout, depression, and late diagnosis (Pearson2021?).
The goal of support is never to produce a person who looks like they don’t have ADHD. It is to produce conditions in which a person with ADHD can do what they are actually capable of, which is often considerably more than the environment has allowed them to demonstrate.
What Not to Say
The following responses to ADHD traits are common and consistently unhelpful. They reflect a misunderstanding of the condition as a motivation problem rather than a neurological reality.
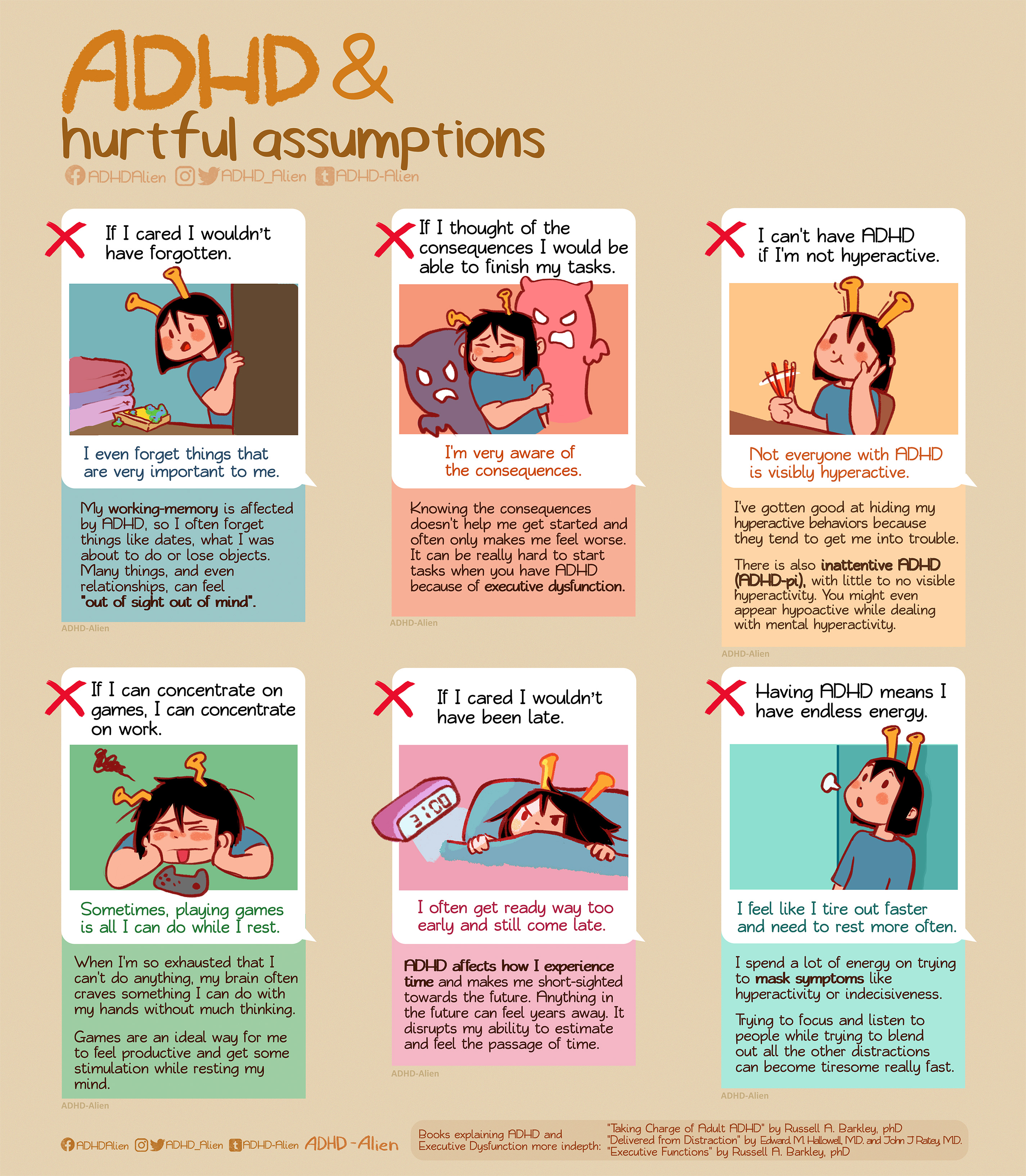
The pattern underlying all of these responses is the same: they locate the problem in the person rather than in the mismatch between the person and the environment. This is not just inaccurate, it actively prevents the kind of structural thinking that would actually improve outcomes.
Recognizing the Cycle
ADHD-related burnout follows a recognizable pattern, and one of the most useful things an ally can do is learn to see it coming rather than responding only once it has arrived.
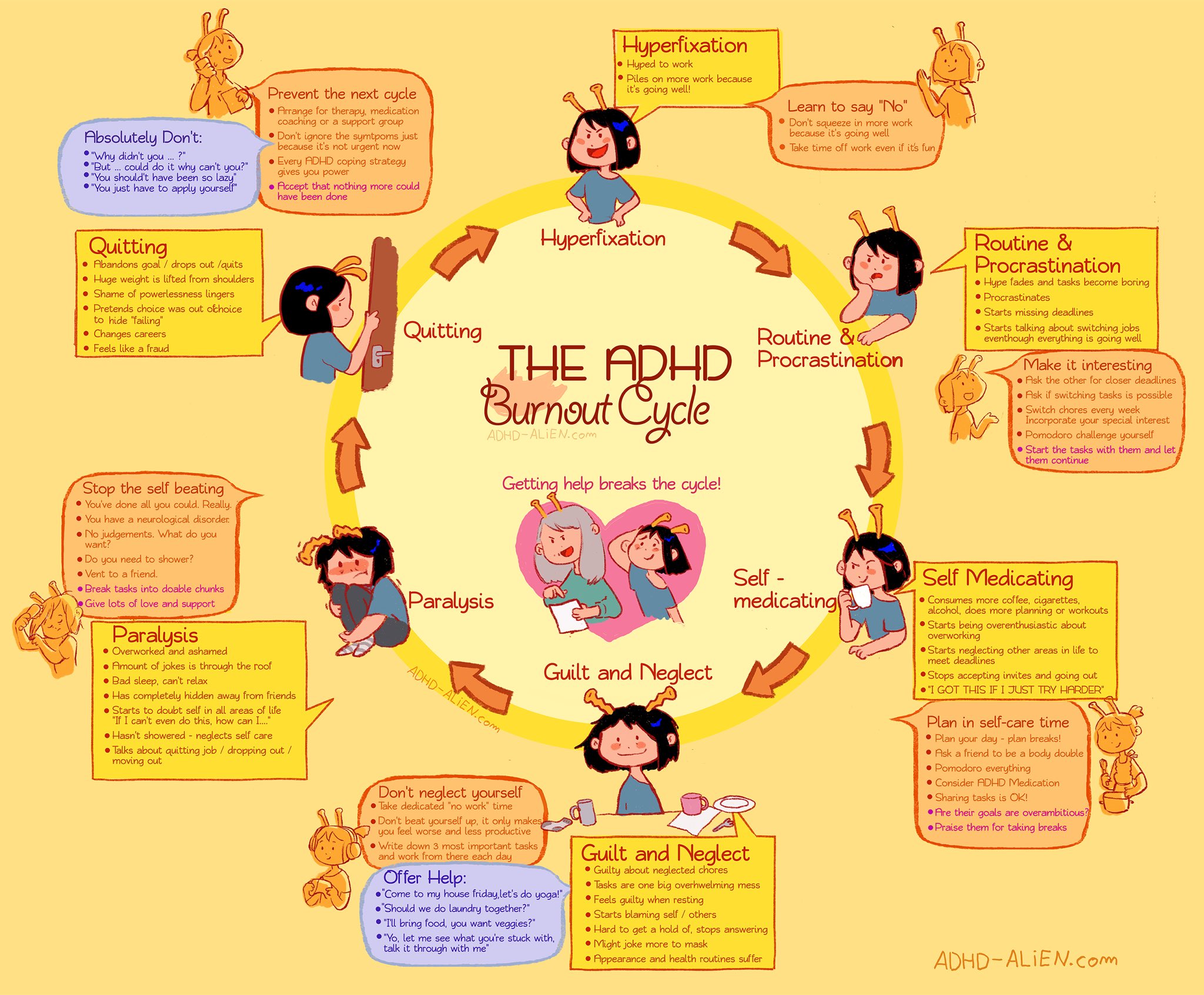
The cycle typically involves a period of high output sustained through masking and compensatory effort, followed by depletion, followed by reduced capacity that gets read as laziness or regression, followed by increased pressure, followed by shame, followed by further depletion. The intervention that breaks the cycle is rarely more effort. It is reduced demand, increased support, and the space to recover without being penalized for needing to.
Recognizing the privilege in how different one’s own reality with work and energy may be, even when two people share the same title, the same workspace, or the same to-do list, is where effective allyship begins. Not in fixing, but in seeing accurately.